
Jia Han Chang, MBChB *, Luke Anthony, MBBS, FRACS
Surgical Division, Mackay Base Hospital, Mackay, Queensland, Australia.
*Corresponding author: Jia Han Chang, 475 Bridge Road, West Mackay, QLD 4740, Australia.
Received date: April 26, 2023
Accepted date: May 01, 2023
published date: May 10, 2023
Citation: Jia H Chang, Anthony L. (2023) “Large Bowel Intussusception Masquerading as Rectal Prolapse”. International Surgery Case Reports, 5(1). DOI: http;//doi.org/05.2023/1.1065.
Copyright: © 2023 Jia Han Chang. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Intussusception is more common in children, and when occurs in adults, this must raise suspicion of an underlying pathology. We present a case which presented with rectal prolapse initially, later finding out to be a descending colon malignancy.
Case Report
55-year-old woman presented to the emergency department with blood-stained mucus discharge per rectum and intermittent lump per rectum for 3 days. She reports this has been happening for the last 3 months and recently had a flexible sigmoidoscopy which showed focal active proctitis in the rectum. This occasion she also complains of colicky lower abdominal pain. Her sister had anal cancer treated with radiotherapy. She has no significant medical history and is a lifelong non-smoker. She has left lower abdominal tenderness on palpation without peritonism. Her laboratory results are unremarkable. CT scan was performed and shows an intussusception of the descending colon into the sigmoid colon. She was taken to operating room, where on table flexible sigmoidoscopy showed a mass at the lead point of the intussusception, and healthy mucosa otherwise. Exploratory laparotomy was performed, confirmed the finding on the CT, the intussusception was carefully reduced, and at the lead point there is a palpable 3cm hard mass with cicatrized overlying serosa in the descending colon. Left hemicolectomy was performed with primary side to side staple anastomosis done. Recovery from surgery was unremarkable and was discharged from hospital at day 6 of admission. Histology shows a T3N0 low grade adenocarcinoma. Staging imaging shows no evidence of metastatic disease. Completion colonoscopy 3 months after surgery shows a patent anastomosis and no other significant disease.

Figure 1: Axial CT imaging showing lead point (red arrow) in upper rectum.

Figure 2: Intraoperative image showing the palpable mass.
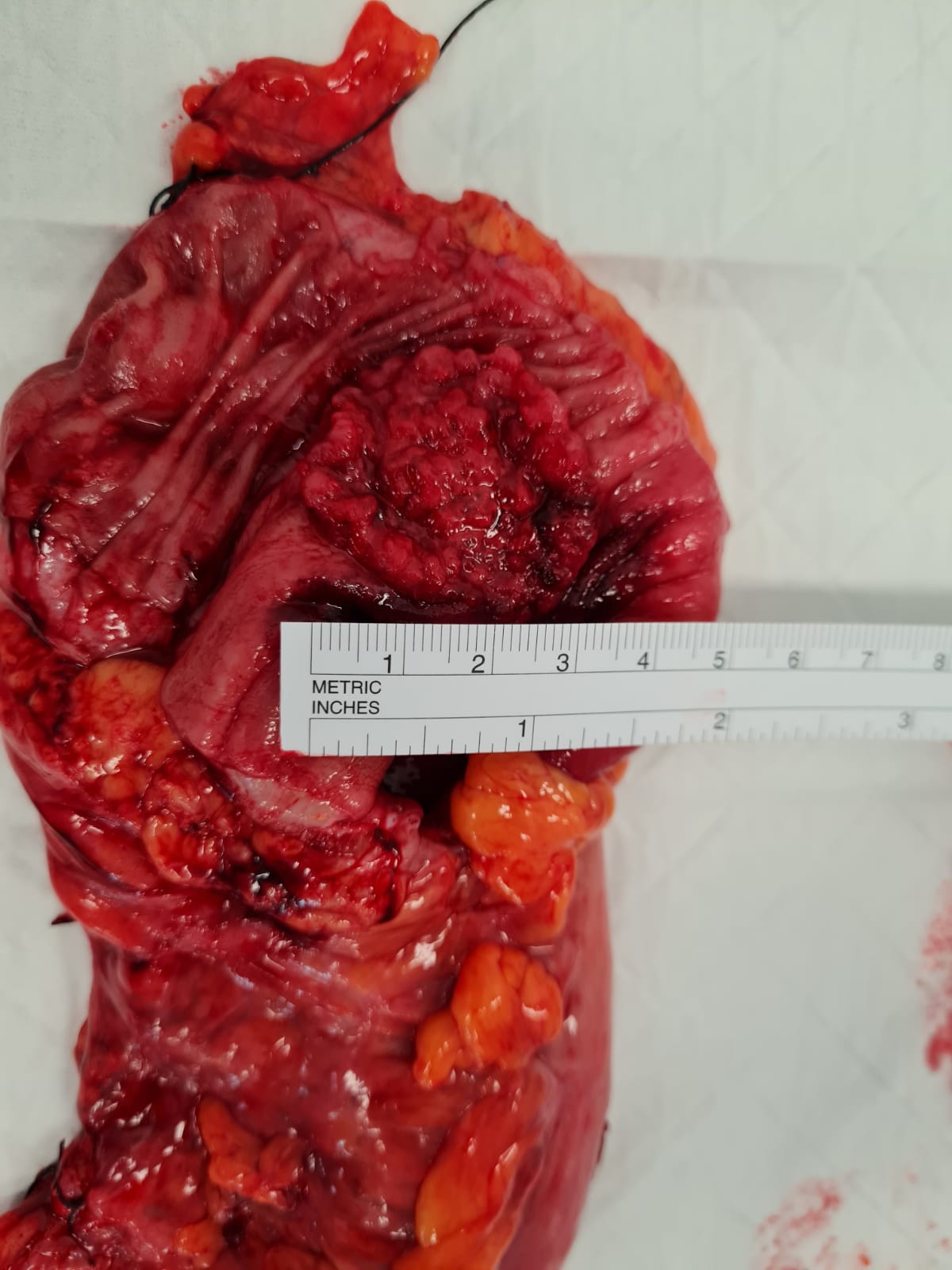
Figure 3: Opened specimen of the left hemicolectomy showing a 3cm fungating mass.
Discussion
Intussusception is the telescoping of a proximal segment of bowel into a distal bowel. This is a rare entity in the adults, only accounting to 5% of all intussusception cases in age older than 18, and approximately 1-5% of adult bowel obstruction. [1-4] 90% of adult intussusception is associated with an identifiable cause, approximately 65% are malignant, most commonly adenocarcinoma of the colon. [3,4] The small bowel is affected more frequently than the colon. [1] Clinical diagnosis is largely difficult given symptoms can be nonspecific, with vague abdominal pain, rectal bleeding, change in bowel habits, or abdominal distension. Most commonly the symptoms are consistent with intermittent partial obstruction, symptoms can be from days to weeks, but rarely chronic. [2,3] Historically, intussusception is only diagnosed is less than half of the cases, however the availability of imaging study has changed this. Whilst plain film X-ray and sonography can help establish the diagnosis, CT is the modality of choice where it is most accurate. [5, 6] While identifying large bowel intussusception is typically possible on CT, identifying the cause remains challenging on imaging, with 69% identified the cause on the series done. [1,5] The other benefit of CT is to provide information for staging as well due to the rate of malignancy. CT finding can also provide information of other complication such as perforation or ischaemia. Given the high rate of malignancy being the aetiology management generally involves surgery. There is no clear consensus about the extent of resection, but in general when there is suspicion that the cause is malignancy, surgeon should strive to perform an oncological resection. The extent of resection is also determined by the viability of the intussusceptum. Limited resection is feasible for benign causes, or when there is a risk of short gut syndrome due to multiple small intestinal polyps [6] Manipulation and reduction is an area of contention however it was suggested not to manipulate due to theoretical risk of intraluminal seeding, perforating the friable and oedematous bowel. [7, 8] Small bowel intussusception on the other hand can be selected for conservative management. Retrospective review identified the definite predictors for surgery on CT was the presence of obstruction, or the presence of a lead point. [9-10]
In our case the presentation masquerading as rectal prolapse could have caused misdiagnosis, led to delayed treatment until further complications has occurred with poorer outcome. It is unusual for the extent of the intussusception that has occurred, and fortunately the intussusceptum showed no ischemia or perforation. It is important to keep a range of differential diagnosis and have appropriate treatment. On table colonoscopy is a reasonable part of the workup for colo-colonic intussusception to obtain information regarding the cause helping to decide on the extend of resection, identify the cause, and the viability of the intussusceptum. However operative management is inevitable given most cases has a cause, and without managing the cause which invariably requires resection intussusception can recur after reduction. When on initial review of a rectal prolapse in the clinic setting, consideration for a complete colonoscopy instead of a limited sigmoidoscopy should be considered, as in our case where the malignancy was missed on sigmoidoscopy due to the malignancy was more proximal than initially expected when the sigmoidoscopy was performed.
Disclosure Statement: No conflict of interest reportable.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org